

It’s shaping up to be a two newsletter day. This will be a quick look back. Black History Month reaches an official end while Black History’s being made ahead. Women’s History Month begins tomorrow and Women’s History is being made in abundance ahead, too.
To commemorate both, take a good look at a slice of the life of the trailblazing Fannie Lou Hamer. Her efforts propelled national attention on the need for enforceable Black civil and voting rights and while she - like the late Congressman John Lewis - suffered permanent injuries throughout her life to gain the prominent Civil Rights Acts of the mid-Sixties, she continued as an advocate for economic rights for the poor while providing grants of land suitable for family gardens to sustain the benefactors of her efforts. Courage, intelligence, persistence and her faith propelled her - and all of us as a civil nation - forward.
Notes on the Pandemic
The Johnson & Johnson one-shot vaccine achieved Emergency Use Approval yesterday in the US. Most of that fresh vaccine supply will enter the vaccine stream in mid to late April but some may arrive by later this week.
It’s been registering a 72% effective rate in US trials, though experts believe with a larger sample size of people using it, that percentage will rise. As it’ll be easier to ship, store and track, it should lead to an increase in distribution centers as clinics and doctor offices should be more able to store and administer the shots.
Health experts fully expect there’ll be more reluctance to get it with 94% or higher effectiveness rates from Pfizer/BioNTech and Moderna vaccines. But with 3 chances out of 4 weighing in our favor, most people shouldn’t hesitate at all. When the US as a whole gets 70% vaccinated, the risk of exposure will fall, raising the success rates even more.
I think it wise to weigh one’s co-morbidity factors before making that choice. If you do decline the J&J shot, when will you get a second choice? If I have multiple co-morbidity factors like obesity, cardiovascular problems, a compromised immune system or work in a frontline position where exposure odds are higher, I might consider holding out for that second choice. I’d have to find out how much longer that wait would be to make a fully informed judgment.
Vulnerable groups have to be their own best frontline defenders.
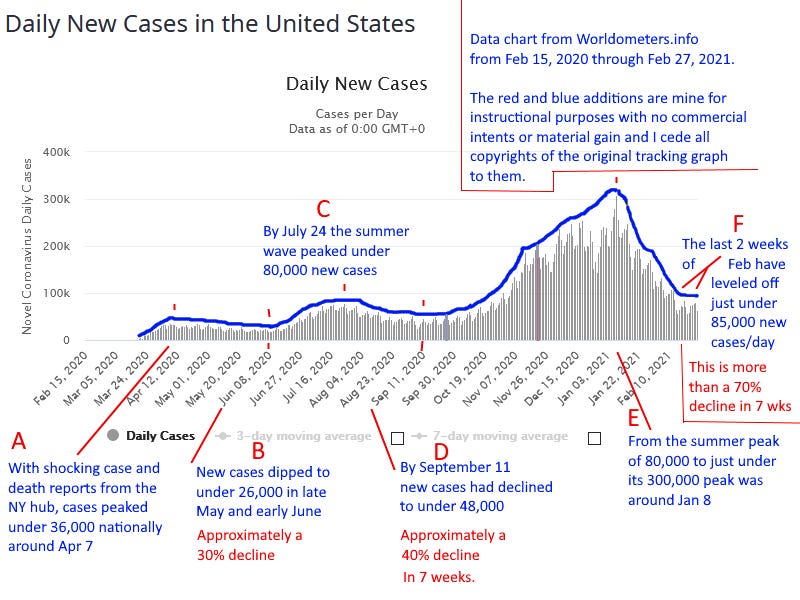
( Chart comes from https://www.worldometers.info/coronavirus/country/us/ with my added red/blue notes for visual aid purposes only. )
__________________________________________________________
We were shocked when the NY hub in the early stage of the first wave exploded with cases and corpses in March and April before testing could begin accurate and effective spread prevention measures. Reopening after 4 or 5 week covid declines of around 30% proved too hasty. The benefit of hindsight indicates 7 weeks of decline is the minimum we need to achieve to assess whether to broaden exposure risks.
Looking at a New Cases chart with the perspective that the April and July highs were one wave rather than two, it took almost 5.5 months to reach the July 24 peak and a similar 5-1/2 months to reach the second peak near Jan 8. Looking forward, the next peak would be due in late June this year if that pattern holds.
Seven weeks after the July peak, we’d seen a 40% decline but it rebounded to astronomical heights over the next 17 weeks. Now we’ve completed another 7 week decline so a rise from here could produce another peak near the end of June. But there are big impediments that will restrict that wave.
A carefully considered guess is that - after the spike from Thanksgiving gatherings and the fall harvest spike in the migrant working families, Christmas plans got scaled back. While airline travel reached the highest level near Christmas since March lockdown measures began in some states, those who traveled were likely to take added precautions due to the escalating numbers. As a result, Christmas surges only occurred in about one-fifth of the states and were shortlived. Early peaks occurred in a few upper Midwest states before November 15th but the last state to peak - Virginia - did so closer to mid January.
Now, Virginia’s death toll was peaking last week, within the standard lag time between the peaks of the new cases and their deadly outcomes. At the national level, we’ve seen a seven wk decline of close to 72%. That’s stunning.
Extra precautions PLUS the escalating vaccine rollout have clearly turned the tide. A third factor in my estimates is some of the most at risk populations - like those residing in care facilities and institutions - have been decimated so there’s fewer people extra vulnerable now that the virus can attack.
I can see some states have reduced their numbers to October levels and a few much lower than that. The national chart has us at late October levels, but some states are barely into November levels. We have to do better, in most states, to suppress any rebounds that I expect will start occurring now.
Our biggest state, CA, remains on track for further decline. It’s too early to make as good an assessment of Texas, as its testing levels and vaccine distribution gets back on track after its climate crisis emergency.
In the next trio of largest states, IL looks okay still while NY and FL are leveling off too high with signs they might begin rebounding. GA, MA and NJ are also displaying early signs of reversal. States that pounce quickly to rein in fresh rises now will likely save more lives.
I finally feel confident that the next wave will be muted, perhaps confined to 3 or 6 week periods in a few states. In most states, the over-60 population will be vaccinated before April and people from 18 to 60 with comorbidity factors will be vaccinated before summer officially begins. Infections can rise without outcomes so dire.
So a large degree of normalcy is achievable by mid-June, where small gatherings between vaccinated households can resume. And none can predict whether all most precautions can be abandoned by Labor Day or whether booster shots will be needed then, like annual flu shots are done now. It’s a pretty amazing vaccine rollout thus far despite the distribution and access problems that some cities or states have experienced.
Our first aim in every state should be to take more precautions - not less - till each state is back to the early September level that state was at. If we proceed with caution and increase our vigilance in March, we’re likely to see end goals come into view after that.
————————————
A Last Look
The $1.9 trillion Covid Rescue package has passed the House. The Senate and President are reasonably confident they can get it fully passed into law in the next two weeks. That’ll leave about 6 weeks in the standard 100 day presidential honeymoon period for other goals like a minimum wage increase, a core infrastructure rebuild plan and others that Biden was elected to do.
The GOP just launched its partisan politics season with CPAC this weekend as it attempts to discredit, derail, impede and reverse any achievements that the moderate Biden has made, just as they’ve done for years with the Affordable Care Act.
If moderates and liberals and independents can sustain the forward momentum through April, the entire country and its economy can see some lasting gains. My next newsletter today will provide the look ahead - as March gains will be crucial toward that aim and it’ll be the best strategies and messaging that will win, not the best intentions alone.
Feel free to share both these outlooks and look both ways before crossing anyone.
Fannie Lou Hamer: “We are sick and tired of being sick and tired.”
When you have the time for a deeper look at Hamer’s efforts, that’s covered very well in this 27 minute video.